
Documentation of Estimated Blood Loss: Consistency Tips for Trauma Patients
Estimating blood loss in trauma care is a bit like estimating how much coffee is left in an opaque travel mug—you think you know, but chances are you’re wrong (and it matters more than you'd like to admit). In trauma settings, consistency in documenting estimated blood loss (EBL) is not only a clinical expectation but a critical patient‑safety behavior. Accurate EBL documentation guides transfusion decisions, informs resuscitation efforts, and supports outcome analysis across systems of care.
However, despite its life‑saving importance, EBL remains notoriously subjective. Research continues to show that humans—regardless of training—tend to underestimate blood loss, especially as the volume increases (French et al., 2020).
And in trauma specifically, EBL is often recorded amidst chaos: rapid assessments, high‑stakes interventions, and unfamiliar or uncontrolled environments.
But with better awareness and a few evidence‑based habits, clinicians can strengthen the reliability of their EBL documentation—and maybe even enjoy it a little.
Why Consistency Matters (And Why It’s Hard)
EBL helps determine whether a patient meets criteria for interventions like massive transfusion, which themselves significantly influence survival (Schneider et al., 2023).
Under‑ or over‑estimating blood loss can shift providers toward inappropriate over‑resuscitation or dangerous delays in transfusion.
Unfortunately, visual estimation—the most common method used in trauma—has been repeatedly proven to be subjective and imprecise (Lin et al., 2024; Stoker et al., 2024).
Even highly trained clinicians show wide variability in their estimates, especially when blood is on clothing, pooled on the floor, mixed with other fluids, or absorbed into linens.
And trauma care rarely offers a neat, non‑absorbent white surface for comparison—wouldn’t that be nice?
EBL Consistency Tips for Trauma Documentation
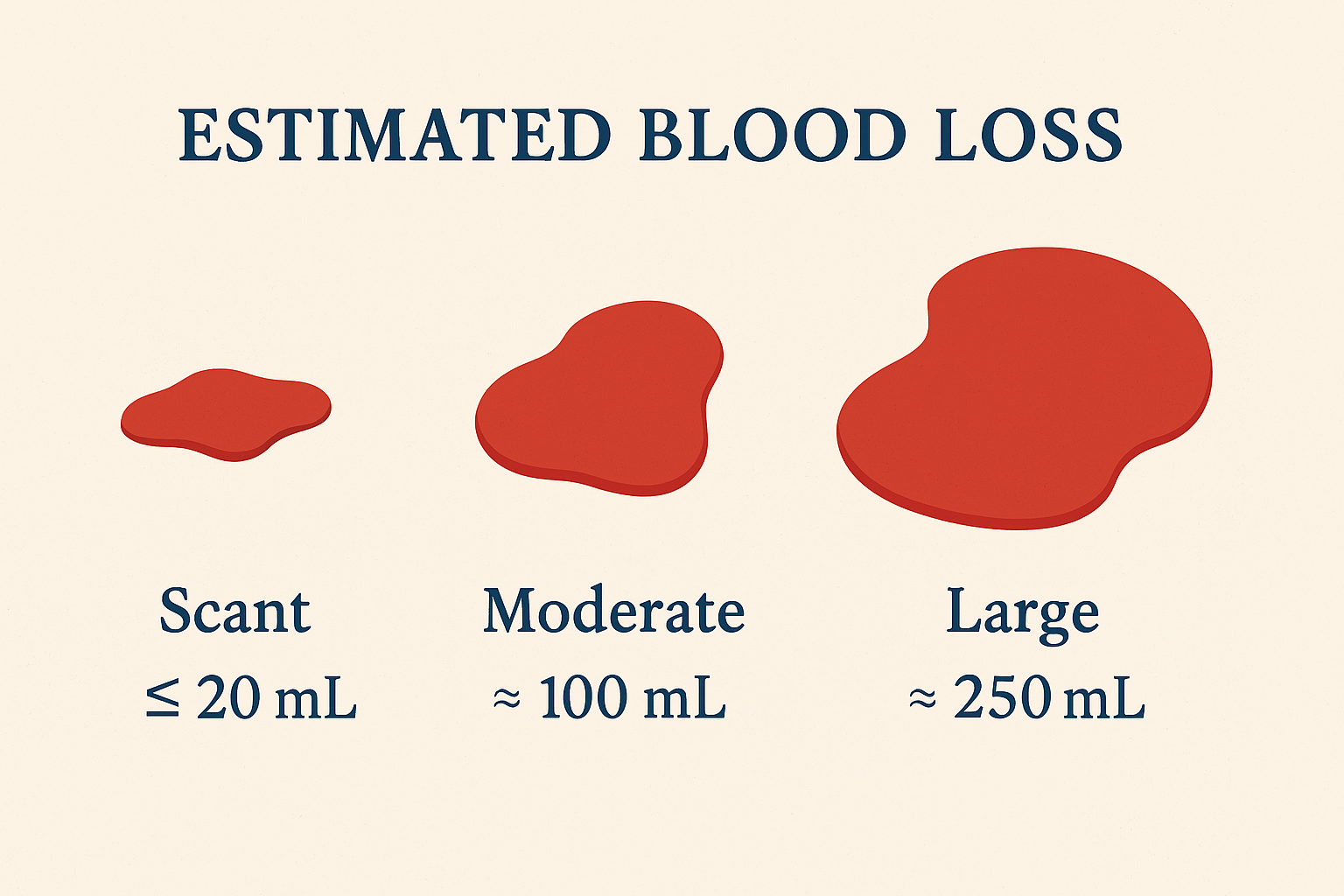
1. Use Standardized Visual Anchors
Studies show that people estimate better when they have reference points (French et al., 2020).
Create quick‑access visual cues in your department—posters showing calibrated blood volumes on common surfaces, or laminated cards in trauma bays.
2. Note the Environment
Blood on asphalt? Clothing? Multiple surfaces? Document where the blood was found. Visual distortions affect accuracy, but calling them out helps future clinicians interpret your estimate.
3. Use Team‑Based Estimation
Two (or more) brains are better than one: collaborative estimation improves accuracy, especially when combining perspectives of EMS, ED, and trauma teams.
4. Lean on Objective Measures When Possible
While trauma rarely allows gravimetric or colorimetric methods, recognizing their superiority reinforces caution when relying solely on visual estimation (Lin et al., 2024).
5. Tie EBL to Vital Signs and Shock Class Trends
Although ATLS shock classes do not perfectly correlate with physiologic changes, trends in heart rate and systolic blood pressure can support your estimation (Guly et al., 2011).
Use them as context—not confirmation.
6. Document Ranges Instead of Absolutes When Appropriate
Instead of “EBL = 300 mL,” recording “Estimated between 250–350 mL based on pooled floor volume” shows thoughtful assessment and limits false precision.
7. Don’t Forget What the Documentation Is Used For
Inconsistent documentation affects quality metrics, trauma registry data, and transfusion‑related benchmarking (Boteilho, 2024).
Your note today may influence a performance improvement project—or a survivor’s long‑term outcome—tomorrow.
An Important Final Reminder
If estimating blood loss makes you feel like you’re auditioning for a forensic TV show, you’re not alone. The key is not perfection—it’s consistency, transparency, and using every tool available to make the estimate as defensible as possible.
Trauma care will always be messy. Your documentation doesn’t have to be.
Commit today to using at least one new consistency strategy in your next trauma EBL documentation.
Educate your team, integrate reference tools into your workflow, and champion accuracy.
Your future patients—and your trauma registry colleagues—will thank you.
References
Boteilho, P. C. (2024). Standardizing massive transfusion protocol documentation: An initiative to improve quality. Oregon Health & Science University. https://digitalcollections.ohsu.edu/record/42890/files/Boteilho.Patti.2024.pdf
French, M. C., Cowling, K., Zyzanski, S., & Ragina, N. (2020). Visual estimation of blood loss. Annals of Emergency Medicine, 76(4), S144. https://www.annemergmed.com/article/S0196-0644%2820%2931135-5/fulltext
Guly, H. R., Bouamra, O., Spiers, M., Coats, T., & Lecky, F. E. (2011). Vital signs and estimated blood loss in major trauma: Testing the validity of the ATLS classification. Resuscitation, 82(5), 556–559. https://doi.org/10.1016/j.resuscitation.2011.01.013
Lin, Y., Yu, C., & Xian, G. (2024). Calculation methods for intraoperative blood loss: A literature review. BMC Surgery, 24, Article 394. https://link.springer.com/article/10.1186/s12893-024-02699-3
Schneider, A. B., Adams, U., Gallaher, J., et al. (2023). Blood utilization and thresholds for mortality following major trauma. Journal of Surgical Research, 281, 82–88. https://www.journalofsurgicalresearch.com/article/S0022-4804%2822%2900530-3/fulltext
Stoker, A. D., Binder, W. J., Frasco, P., et al. (2024). Estimating surgical blood loss: A review of current strategies. SAGE Open Medicine, 12, Article 20503121241308302. https://doi.org/10.1177/20503121241308302