
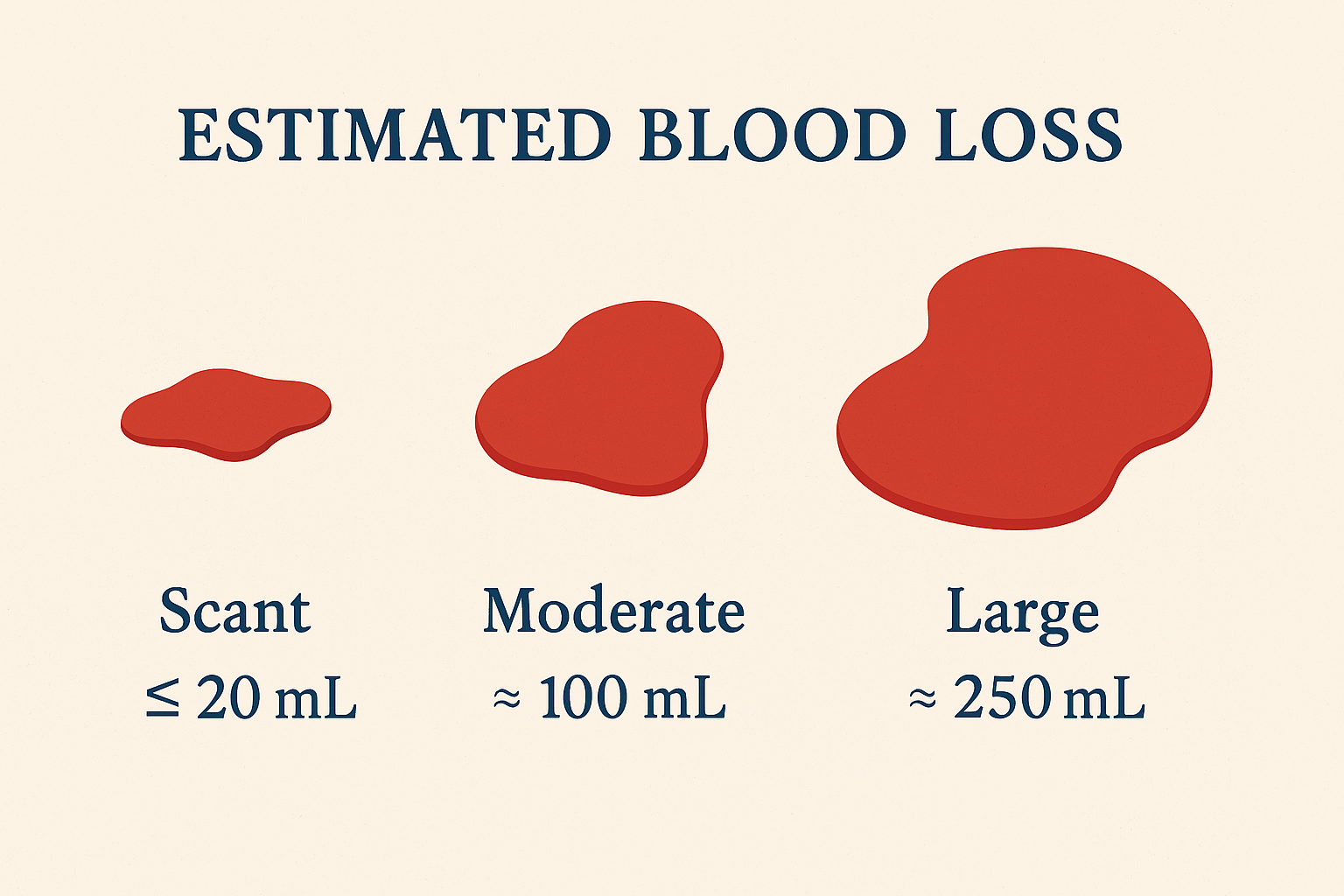
Documentation of Estimated Blood Loss: Consistency Tips for Trauma Patients
Estimating blood loss in trauma care is a bit like estimating how much coffee is left in an opaque travel mug—you think you know, but chances are you’re wrong (and it matters more than you'd like to admit). In trauma settings, consistency in documenting estimated blood loss (EBL) is not only a clinical expectation but a critical patient‑safety behavior. Accurate EBL documentation guides transfusion decisions, informs resuscitation efforts, and supports outcome analysis across systems of care.

The Impact of Delays (Non-clinical)—Time to Intervention in Trauma
When it comes to trauma care, speed is the closest thing we have to a superpower. Unfortunately, the real world is not a Marvel movie, and delays—particularly non‑clinical ones—can turn what should be a smooth rescue mission into a bureaucratic obstacle course. Research consistently highlights that delays along the trauma care continuum—from incident to imaging to surgery—are associated with decreased survival, demonstrating how time‑critical trauma truly is.

The Pelvis: The Quiet Overachiever of Trauma Bleeding
If the human body hosted a talent show, the pelvis would never seek the spotlight—yet it would quietly steal the show by holding vital structures together, transmitting force, and, in trauma, hiding enough blood loss to make even seasoned clinicians uneasy. Pelvic injuries may appear subtle on the surface, but beneath the skin they can unleash life-threatening hemorrhage with remarkable efficiency. In trauma care, underestimating the pelvis is not just an error—it’s a gamble with physiology.
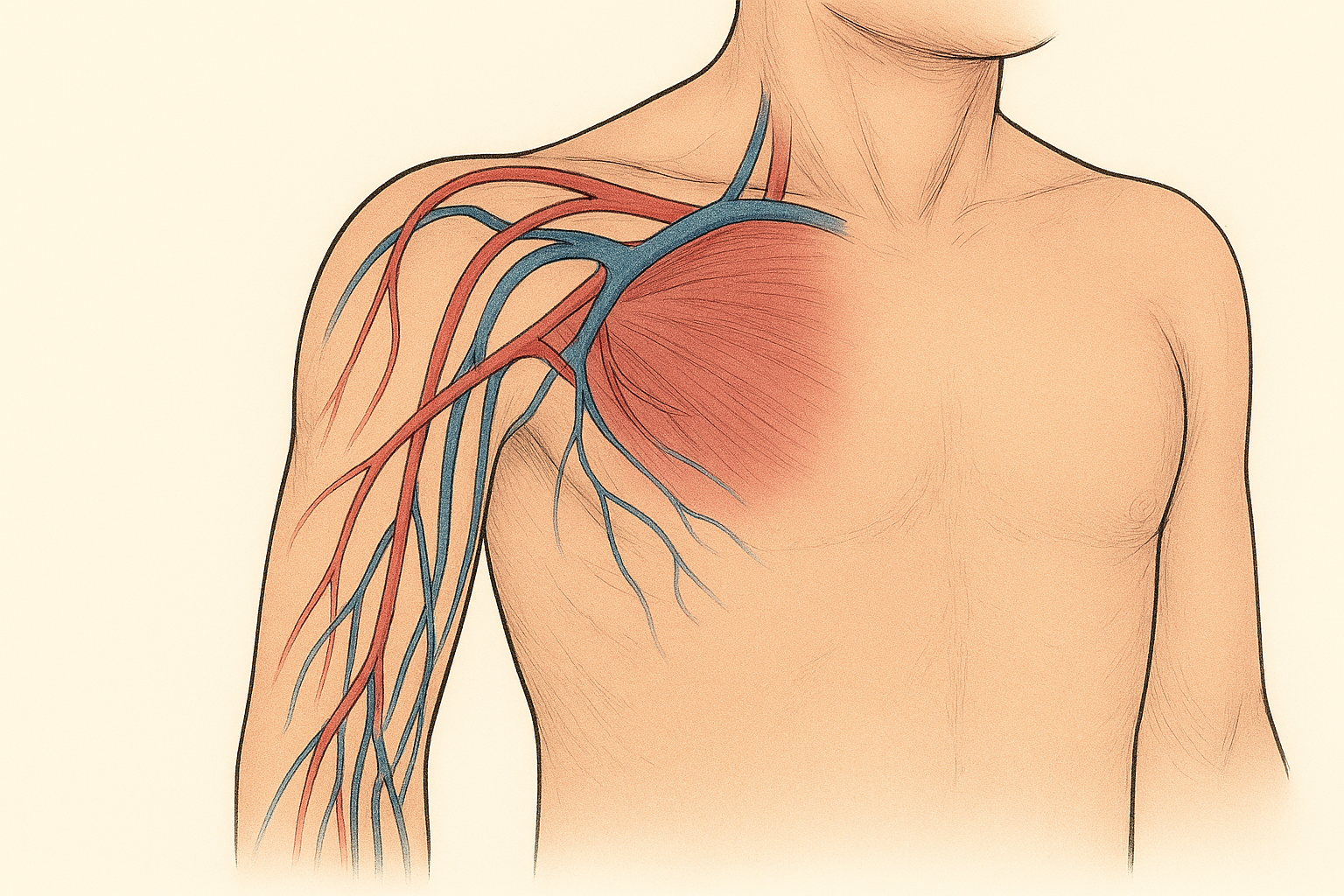
Junctional Bleeding: Why Trauma’s Most Awkward Real Estate Still Wins Fights
If hemorrhage control were a dinner party, extremity bleeding would be the polite guest—easy to seat, easy to manage, perfectly content with a tourniquet. Junctional bleeding, on the other hand, shows up uninvited, wedges itself between the torso and limb, and refuses every polite intervention you brought. It’s trauma’s most inconvenient problem—and the more we fix extremity bleeding, the more junctional hemorrhage steps into the spotlight (Kotwal et al., 2013; van Oostendorp et al., 2016).
What is it? Bleeding at the “hinge points”—groin, axilla, perineum, buttocks, and base of the neck—where large vessels run deep and circumferential compression just doesn’t work. In modern systems, junctional and truncal bleeding remain among the leading causes of potentially preventable death, often occurring before patients reach definitive care (Kotwal et al., 2013; van Oostendorp et al., 2016).

Tourniquets: Indications (Concept Only)
When compression is not just a hug, but a life-saving decision
Tourniquets have had a remarkable public relations comeback. Once feared as limb-dooming relics of bygone medicine, they are now celebrated as decisive tools against one of trauma care’s most unforgiving enemies: uncontrolled hemorrhage. Thanks to modern evidence, military experience, and public health campaigns like Stop the Bleed, tourniquets have moved from the margins to the mainstream. Still, the key to their benefit lies not in enthusiasm, but in indication—knowing when a tourniquet is conceptually appropriate, and just as importantly, when it is not (Mikdad et al., 2021).

From Bystander to Lifesaver: Why ‘Stop the Bleed’ Belongs in Everyone’s Skill Set

Hemorrhage in Trauma: What You See Can Kill—And What You Don’t See Can Kill Faster
Hemorrhage in trauma is like an iceberg: the visible portion may be dramatic, but it is often the unseen mass below the surface that sinks the ship. After central nervous system injury, hemorrhage is the leading cause of preventable death in trauma patients, with many fatalities occurring within the first two hours of injury (Latif et al., 2023). Knowing where bleeding comes from—and how it presents—is critical to saving lives.

Massive Transfusion in Trauma: A Team Sport Played at Sprint Speed
Hemorrhage remains the leading cause of preventable death after trauma, and when it strikes, it does so without RSVP. Massive transfusion is not a solo act—it is a tightly choreographed, multidisciplinary performance where timing, communication, and role clarity decide whether the patient gets a standing ovation or the curtain falls too early (American College of Surgeons [ACS], 2014; Meneses et al., 2020). A well-designed Massive Transfusion Protocol (MTP) transforms chaos into coordinated care, aligning the trauma bay, operating room, blood bank, and support services around a single goal: rapid hemorrhage control with hemostatic resuscitation (Holcomb et al., 2015; International Society of Blood Transfusion [ISBT], 2026).
This article offers a professional, practical, and slightly witty overview of trauma team workflow during massive transfusion—because saving lives is serious work, but clarity doesn’t have to be dull.
Lactate and Base Deficit Walk Into a Trauma Bay
In trauma care, numbers speak—sometimes more honestly than patients can. Among the most talkative are serum lactate and base deficit. They don’t give orders, write protocols, or replace clinical judgment, but they do whisper (and occasionally shout) important truths about tissue perfusion, physiologic stress, and the body’s ongoing negotiation with shock. Understanding what these markers suggest is essential for trauma clinicians who want to read between the vital signs.
The Quiet Creep of Shock: Catching the Subtle Vital Sign Clues in Trauma Activations
Shock rarely announces itself with sirens. In the trauma bay, it often tiptoes in—polite, quiet, and dangerously convincing. Blood pressure looks “okay.” The patient is talking. The monitor hums along, unimpressed. And yet, somewhere between the triage vitals and the first CT slice, physiology is slipping. Early shock recognition is less about dramatic numbers and more about trends, context, and a healthy distrust of “normal.”
This article explores the subtle vital sign patterns that precede overt decompensation in trauma activations—and how clinicians can spot trouble before the crash cart earns its keep.

Clear Notes, Clear Minds: The Power of Time‑Anchored Narrative Documentation in Trauma Activations
Trauma activations are the medical equivalent of controlled chaos—fast, noisy, and full of life‑or‑death decision‑making. Amid the swarm of assessments, interventions, and team communication, one thing must remain calm, consistent, and crystal‑clear:
The documentation.

Tick‑Tock Trauma: Why Clock Synchronization Matters More Than You Think
Trauma activations move fast—so fast that seconds can feel like plot twists. In these high‑stakes moments, monitors beep, staff shout updates, labs run, medications fly, and documentation becomes the anchor that holds the story together. But there’s one tiny detail that often sneaks under the radar:
Are your clocks even telling the same story?

Time, Dose, Action: Making Medication Documentation in Trauma Activations Make Sense
In trauma care, medications don’t simply happen—they happen at a moment, for a reason, and with consequences. Capturing the timing of those medications and linking them to the events unfolding in the trauma bay is not just administrative diligence; it is the backbone of accurate care documentation, trauma registry abstraction, and quality improvement. And let’s be honest: without good timestamps, even the most heroic interventions can read like a script with half the dialogue missing.

The Art and Science of Start/Stop Documentation in Trauma Activations
Trauma activations are not only high‑stakes clinical events—they’re also stopwatch moments. Every second counts, and every second must be documented. Within the controlled chaos of resuscitation, accurate procedure start and stop times serve as the quiet heroes of compliance, performance improvement, and trauma center verification. Think of them as the timestamps that keep your trauma narrative from turning into an unintelligible thriller.

Vital Sign Sequence & Timing for Trauma Activations
Trauma activations move fast—so fast that even your caffeine struggles to keep up. In the organized chaos of the trauma bay, vital signs are not just numbers; they are the early warning system, the clinical plot twists, and the data breadcrumbs that guide life‑saving decisions. But timing and sequence matter. Document them well, and you look like a resuscitation rockstar. Document them poorly… and quality audits will find you in the chart review dungeon.
This article dives into the why, what, and how of proper vital sign sequencing and timing during trauma activations—bringing evidence, wit, and a gentle nudge to tighten up documentation habits.

Trauma Bay Readiness: Because Chaos Deserves a Well‑Organized Stage
If the emergency department (ED) were a theatre, the trauma bay would be its high‑stakes main stage—where the script is unpredictable, the stakes are life‑and‑death, and the actors are expected to perform flawlessly under pressure. Trauma bay readiness is not optional; it is the backbone of safe, effective trauma care. And like any great production, readiness hinges on planning, practice, and having the right equipment in the right place at the right time.

Debrief Touchpoints Post‑Activation: Building Culture One Conversation at a Time
In trauma care, chaos is a given—but culture is a choice. Amid the bright lights, pagers, and the unmistakable hum of urgency, trauma teams perform under extraordinary pressure. But what happens after the adrenaline dissolves? That’s where debrief touchpoints step in: the structured moments that transform good teams into exceptional ones and turn high‑stress events into high‑value learning and connection.

Family Updates in Trauma Care: Who, When, and How—A Principles‑Driven Guide
When trauma strikes, families don’t just want information—they need it with the urgency of someone refreshing a package‑tracking page every 20 seconds. The emergency department is a whirlwind of assessments, alarms, and acronyms, and families often find themselves standing at the edge of this storm with one pressing question: “What’s happening?”

Safety in the Trauma Bay: Space Management & Role Discipline When Seconds Count
In trauma care, chaos is a given—but disorganization doesn’t have to be. The trauma bay is a pressure cooker of noise, urgency, and bodies in motion. Without deliberate space management and role discipline, even a well-trained team can devolve into a tangle of elbows, equipment, and crossed responsibilities. As recent literature shows, structure isn’t just nice to have—it’s lifesaving.
