
Loop Creep in Trauma PI: When “Closing the Loop” Starts Running the Show
By design, trauma performance improvement (PI) is a disciplined march from problem identification to problem resolution. By accident, it can become a never‑ending relay race where the baton keeps getting passed but never put down. Welcome to loop creep.

Just Because You Can Close the Loop Doesn’t Mean You Should
Closing the loop is a means, not an end. When done prematurely or inappropriately, it risks undermining learning, distorting culture, and giving a false sense of improvement. In short: some loops should stay open—at least for a while.
This article explores when not to close the loop in trauma PI, and why restraint can be a hallmark of a mature, high-functioning program.

If It Isn’t Documented, It Didn’t Improve: Using Documentation to Prove Closure in Trauma Performance Improvement
Trauma performance improvement (PI) is often described as a “loop,” yet many programs struggle not with identifying issues, but with proving that the loop was actually closed. The uncomfortable truth is this: excellent clinical care without excellent documentation may as well be a rumor. In trauma PI, documentation is not clerical busywork—it is the tangible evidence that improvement occurred, lessons were learned, and patients benefited.
Closing the loop in trauma PI requires more than corrective action; it requires clear, consistent, and defensible documentation that tells the story from identification to resolution. When done well, documentation demonstrates accountability, regulatory compliance, and a mature culture of safety (American College of Surgeons [ACS], 2022).
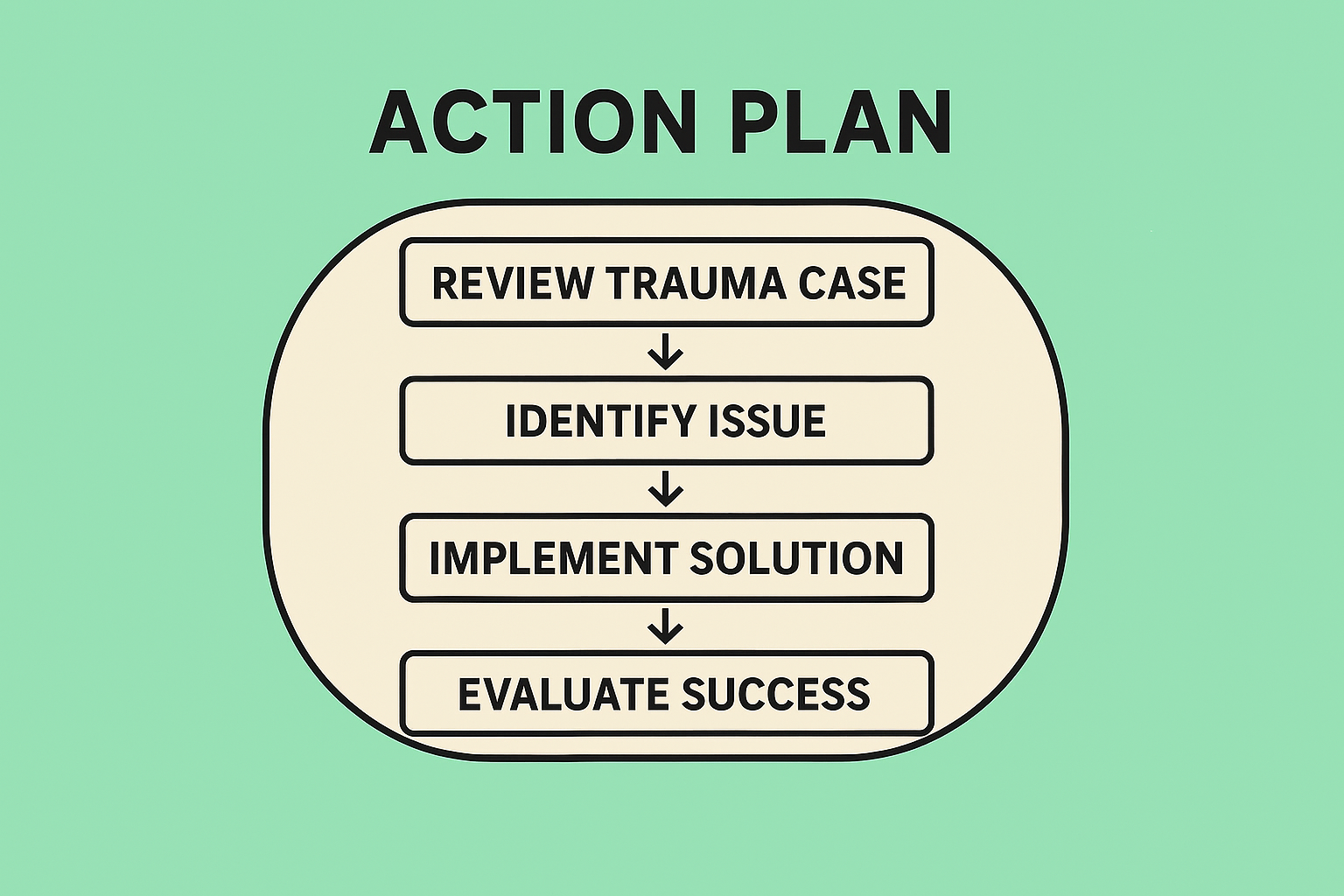
Evidence of Action Plans in Trauma Performance Improvement: When “We Talked About It” Is No Longer Enough
In trauma performance improvement (PI), identifying a problem is the easy part. Documenting an action plan is the expected part. Demonstrating evidence that the action plan actually worked—that’s where many trauma programs start to sweat, usually about three weeks before a verification visit.
The American College of Surgeons (ACS) has been clear: performance improvement and patient safety (PIPS) is not a paperwork exercise. It is a closed-loop system designed to prevent harm to future similar patients (American College of Surgeons [ACS], 2022). In other words, trauma PI is not about proving that you noticed a problem—it is about proving that you changed something and that the change mattered.

How to Write a Strong PI Loop in Trauma
In trauma care, few things inspire as much collective groaning as the phrase “please demonstrate loop closure.” Yet the performance improvement (PI) loop is not merely a regulatory hoop—it is the mechanism by which adverse events become safer systems. A well-written PI loop demonstrates that a trauma program can identify a problem, correct it, and verify that the correction actually worked.

Mind the Gap: Practical (and Painless) PI Loop Closure Timeline Examples
Performance Improvement (PI) has matured. What once passed as “closing the loop” (a meeting note and a hopeful nod) is no longer sufficient in an era of real‑time dashboards, implementation science, and increasingly sophisticated accreditation reviews. Today, loop closure is expected to demonstrate measured change, sustained performance, and learning over time—not just good intentions.
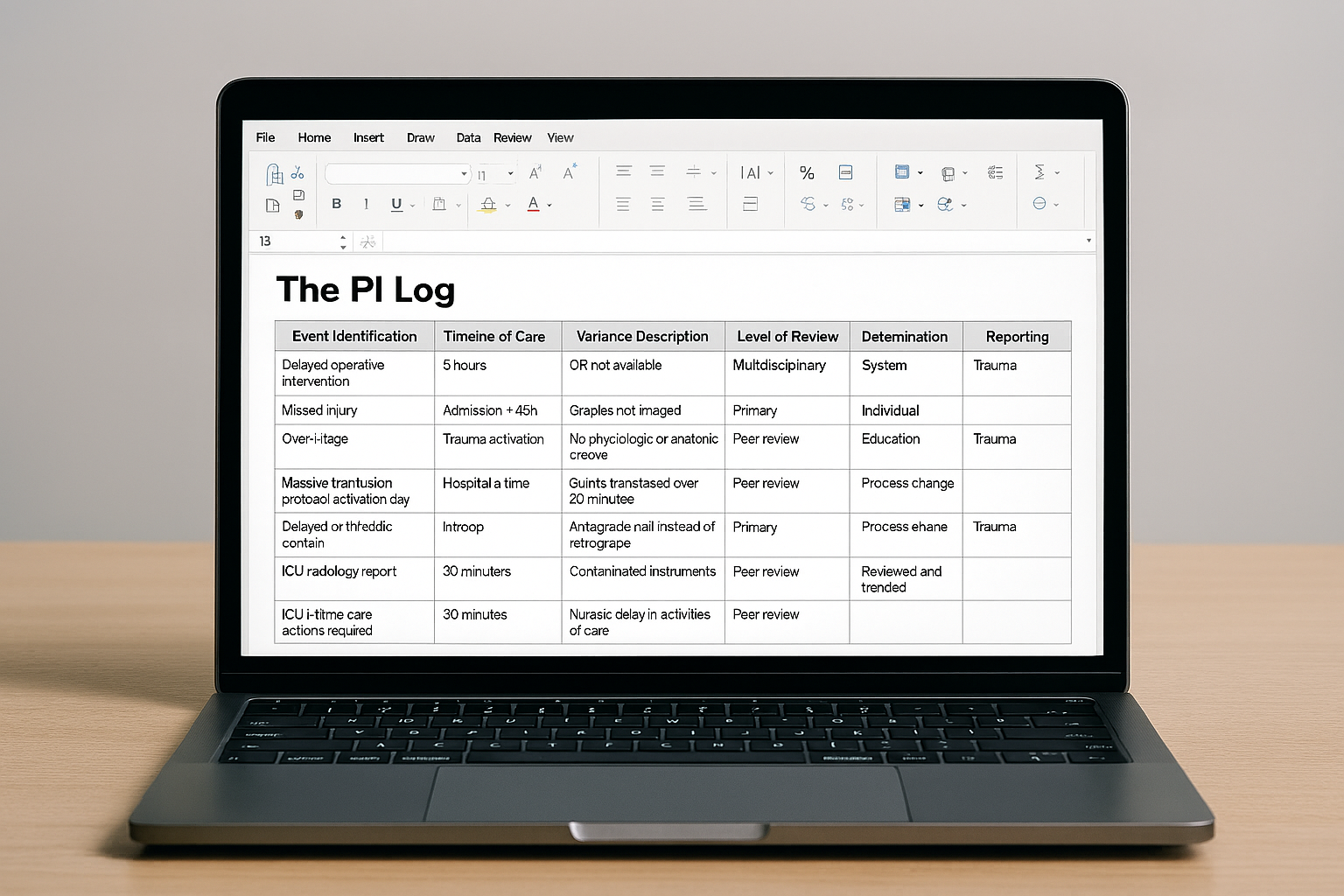
The PI Log: What to Track for Trauma Services (and Why It Matters More Than You Think)
In trauma care, excellence is rarely accidental. It is documented, reviewed, debated, re‑educated, and—eventually—improved. At the center of this continuous cycle lives a deceptively humble tool: the Performance Improvement (PI) log.
Often underestimated (and occasionally feared), the PI log is not merely a list of “who messed up.” When used correctly, it is the trauma program’s early warning system, accountability ledger, and roadmap for safer care—all in one spreadsheet (or database, if you’re living the dream).
So what should a trauma PI log actually track? And how do we ensure it supports improvement rather than becoming a compliance chore? Let’s break it down.

Raising the Right Cases: Smart Escalation in Trauma Peer Review
Trauma care is fast, unforgiving, and occasionally humbling. Even in the best trauma centers, not every case ends with a textbook outcome—and not every deviation from the plan is a failure. The challenge for trauma programs is knowing when a case represents natural clinical complexity and when it signals an opportunity for improvement that warrants escalation to peer review.

The TMD Effect: Why Performance Improvement in Trauma Starts at the Helm
Trauma care is fast, complex, and unforgiving of system failure—yet it is uniquely positioned for improvement when leadership is intentional. Enter the Trauma Medical Director (TMD): part clinician, part strategist, and full‑time steward of quality. While Performance Improvement (PI) in trauma is often perceived as a regulatory requirement, when driven by an engaged TMD, it becomes something far more powerful—a mechanism for safer care, better outcomes, and resilient teams.
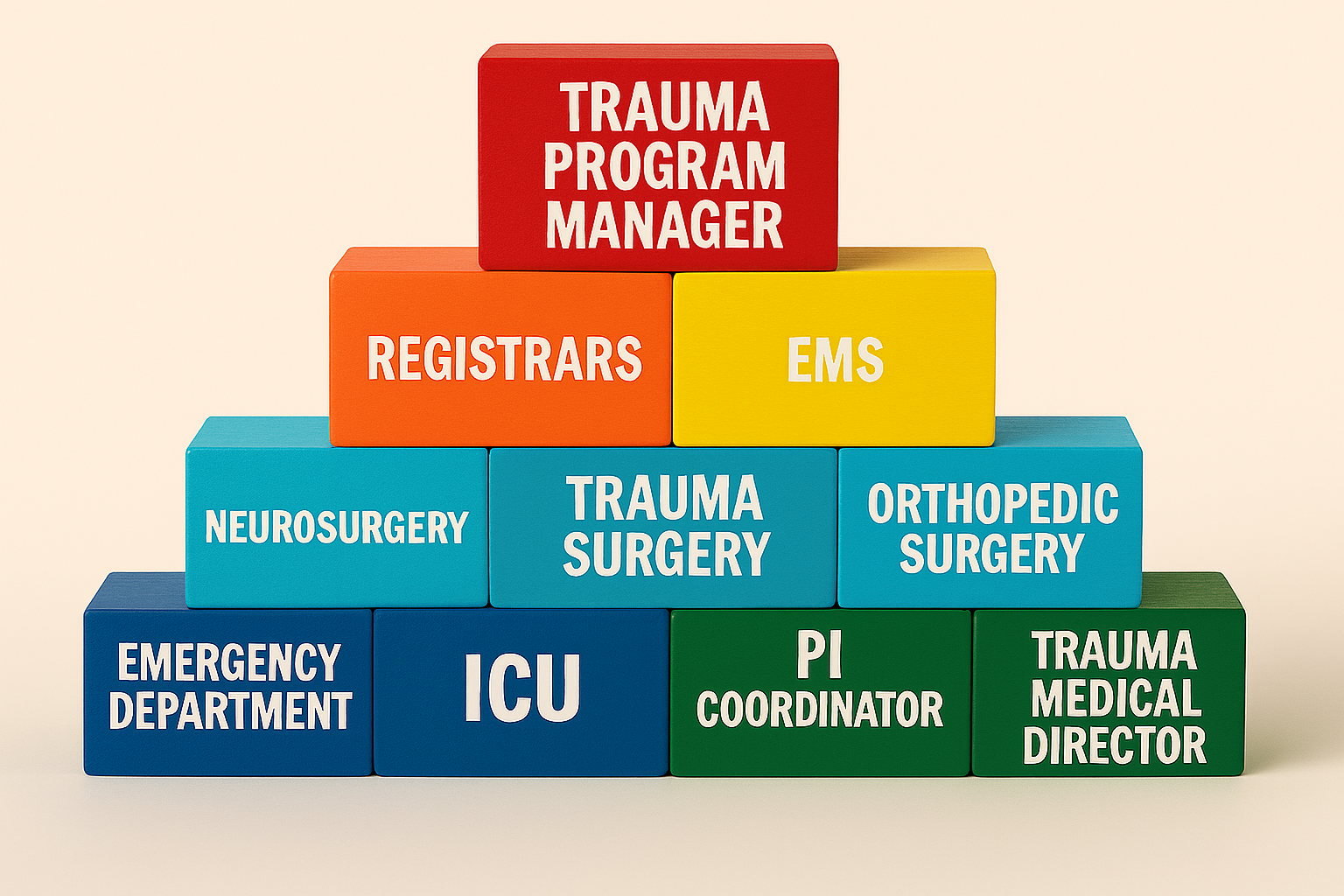
The PI Committee Structure in Trauma: Where Serious Work Meets Seriously Good Structure
Trauma care is not for the faint of heart—but neither is the structure behind the scenes keeping it all running smoothly. Enter: the Performance Improvement (PI) Committee, the engine in the background ensuring trauma programs don’t just function but truly excel. If trauma resuscitation is the dramatic front-of-house performance, the PI committee is the backstage crew pulling ropes, adjusting lights, and occasionally whispering, “Let’s not do that again.”

Closing the Loop Like a Pro: What Good PI Loop Closure Really Looks Like in Trauma Care
In trauma care, “loop closure” may sound like something you do when you finally zip up that overstuffed trauma binder—but in reality, it's the gold standard of performance improvement (PI). It’s the difference between identifying a problem and actually fixing it. Without loop closure, PI is just a very detailed complaint box. With it, PI becomes a powerful engine for better outcomes, safer systems, and fewer “how did this happen again?” moments.

PI vs. QI in Trauma Care: Same Battlefield, Different Missions
In the high‑stakes world of trauma care, where seconds matter and documentation can feel like a full‑contact sport, two champions of better outcomes often get confused for one another: Performance Improvement (PI) and Quality Improvement (QI). They may sound like siblings who steal each other’s clothes, but in practice, they play distinct—and equally essential—roles on the trauma team.
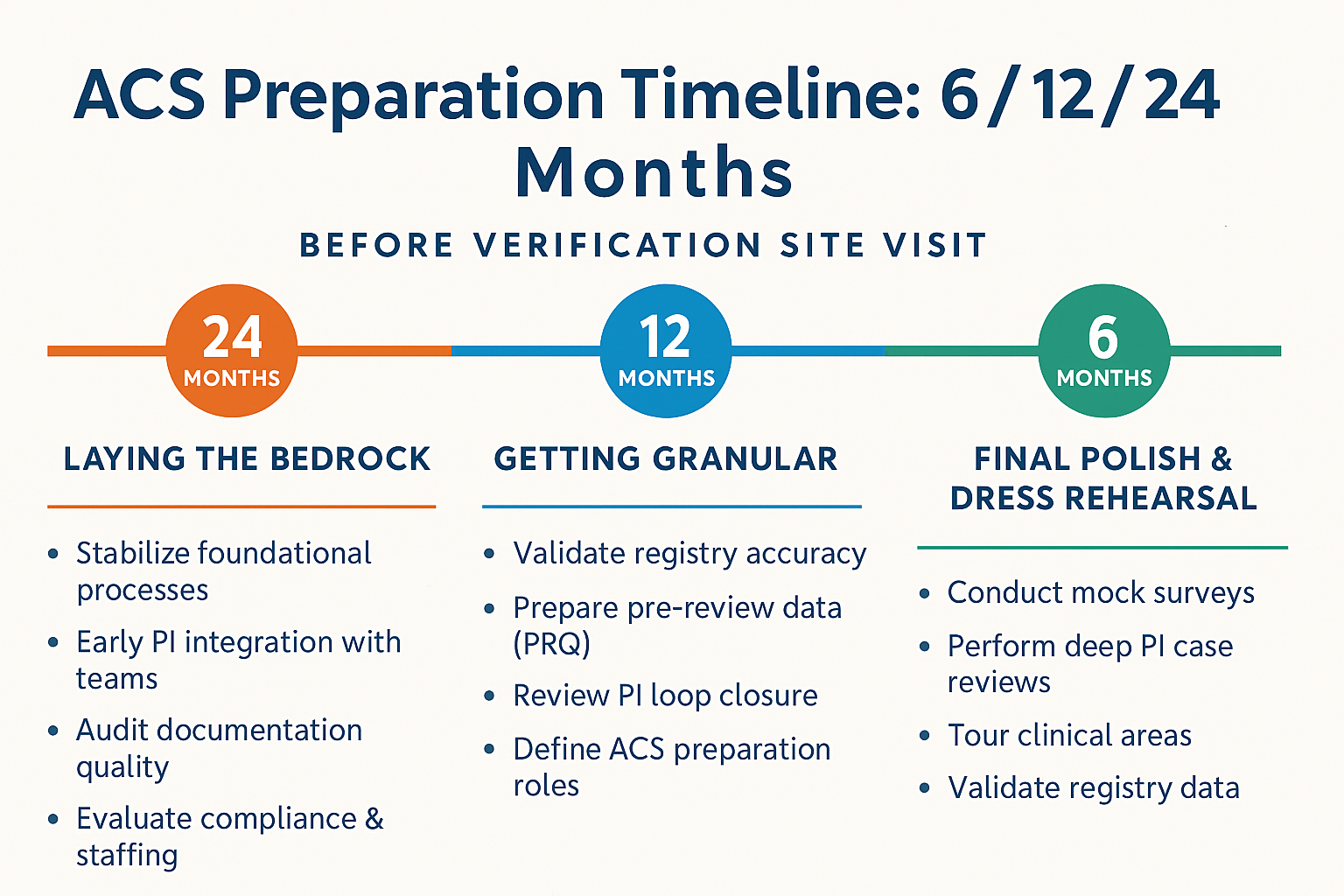
The ACS Preparation Timeline: 6, 12, and 24 Months Out

Talking Trauma: How to Communicate ACS Readiness Without Losing Your Sanity (or Your Staff)
Preparing for an American College of Surgeons (ACS) trauma verification can feel a bit like prepping for a surprise celebrity visit: the house (your hospital) must be spotless, the guests (your staff) should know their lines, and everyone needs to pretend they haven’t been living on caffeine and good intentions for months.
But ACS preparation doesn’t have to be a stress‑inducing, caffeine‑driven scavenger hunt. With the right communication strategy, hospitals can guide staff through the process with humor, clarity, and confidence—all while meeting the rigorous expectations set by the ACS.
ACS Verification Binders: Digital vs. Physical — Which One Deserves the Trauma Crown?
If you’ve ever prepared for an ACS (American College of Surgeons) verification visit, you already know the emotional journey: a caffeine‑fueled odyssey filled with tabs, hyperlinks, frantic file‑hunting, and the occasional existential crisis. Among the many decisions trauma programs face, one question divides coordinators faster than an unexpected tracer question:
Should your ACS Verification Binder be digital or physical?

Trauma Team Documentation: Turning Organized Chaos into a Defensible, Data‑Driven Narrative
When a trauma alert tones out, the room becomes an orchestra at fortissimo: a chorus of vitals, the staccato of orders, and the bass line of critical decisions. In that score, documentation is the sheet music—without it, the performance falls apart. Accurate, timely notes aren’t busywork; they are patient safety, quality improvement, and medico‑legal armor rolled into one (American College of Surgeons Trauma Quality Programs [ACS TQIP], n.d.; American College of Emergency Physicians, 2023).

ICU Requirements in ACS Trauma Verification: Where Precision Meets Controlled Chaos
When it comes to trauma care, the Intensive Care Unit (ICU) is the high‑stakes arena where precision medicine and controlled chaos coexist in a delicate truce. For hospitals seeking trauma verification through the American College of Surgeons (ACS), meeting ICU requirements isn’t just about checking boxes—it’s about demonstrating a system ready to deliver high‑level care when life’s plot twists get a little too dramatic.

Laboratory & Transfusion Requirements in Trauma Care: Precision Under Pressure
Trauma resuscitation is medicine’s ultimate stress test: physiology unravels, time compresses, and decisions ripple across outcomes. In this high‑stakes setting, laboratory data and transfusion requirements are not optional accessories—they’re the GPS, guardrails, and gas pedal for care. The American College of Surgeons (ACS) sets the bar for trauma center readiness, including what your lab and blood bank must deliver when hemorrhage calls the shots (ACS, n.d.).

Scalpels on Standby: Understanding ACS‑Aligned OR Response Requirements for Trauma Patients
When a trauma patient rolls through the doors, the clock doesn’t just start ticking—it starts shouting. In high‑acuity care, the Operating Room (OR) isn’t merely a destination; it’s a promise. A promise of rapid intervention, disciplined coordination, and an entire clinical team spring‑loaded to act. While the American College of Surgeons (ACS) provides the gold standard framework for trauma center readiness, specific expectations around OR responsiveness can be illuminated through state‑level interpretations and complementary trauma system guidelines inspired by ACS principles.
Radiology Requirements for ACS Trauma Verification: Because Trauma Doesn’t Wait for Office Hours
Radiology may not wear a cape, but in the world of ACS Trauma Verification, it absolutely plays the hero. Whether identifying hidden hemorrhage, mapping organ injury, or guiding the surgeon’s next move, radiology is the quiet giant behind trauma care excellence. The American College of Surgeons (ACS) makes this crystal clear in its Resources for Optimal Care of the Injured Patient—the rulebook every trauma center lives by (ACS, 2025a).