
Hemorrhage in Trauma: What You See Can Kill—And What You Don’t See Can Kill Faster

External vs. Internal Hemorrhage Awareness
Hemorrhage in trauma is like an iceberg: the visible portion may be dramatic, but it is often the unseen mass below the surface that sinks the ship. After central nervous system injury, hemorrhage is the leading cause of preventable death in trauma patients, with many fatalities occurring within the first two hours of injury (Latif et al., 2023). Knowing where bleeding comes from—and how it presents—is critical to saving lives.
This article distinguishes external and internal sources of hemorrhage in trauma, emphasizing situational awareness, clinical vigilance, and prompt intervention. Because in trauma care, blood doesn’t wait.
External Hemorrhage: The Bleeding That Demands Attention
External hemorrhage is the bleeding you can see, hear, or sometimes feel squishing through your gloves. It is dramatic, urgent, and—fortunately—often controllable with immediate action.
Common Sources
External hemorrhage typically originates from:
Extremity injuries (arterial or venous)
Scalp and facial lacerations
Junctional wounds (neck, axilla, groin)
Traumatic amputations
These sources are emphasized early in trauma algorithms because uncontrolled external bleeding is a leading cause of prehospital death (American College of Surgeons Committee on Trauma [ACS COT] et al., 2023).
Why It Matters
External hemorrhage is responsible for a substantial portion of preventable deaths, particularly before hospital arrival (Berry & Fischer, 2025). The good news? Timely interventions such as direct pressure, wound packing, and tourniquet application are highly effective when performed early (ACS COT et al., 2023).
The Clinical Pearl
If you can see the blood, stop it first. Airway and breathing mean little if circulation is rapidly leaving the body.
Internal Hemorrhage: The Silent (and Sneaky) Killer
Internal hemorrhage is bleeding that hides behind intact skin, polite vital signs, and a deceptively calm patient. It is less obvious—and often more lethal if missed.
Common Locations
Major internal hemorrhage typically occurs in:
Chest (hemothorax)
Abdomen (solid organ or vascular injury)
Pelvis
Retroperitoneum
Long bones (especially femurs)
These regions can each accommodate large volumes of blood without external signs, earning internal hemorrhage its reputation as a “silent killer” (Nickson, 2020).
Why It Matters
Internal bleeding is frequently underrecognized, even by experienced clinicians. Studies show that major hemorrhage is missed in a significant proportion of trauma patients, particularly those with abdominal or penetrating injuries (Wohlgemut et al., 2024). Hypotension, when it finally arrives, is a late and ominous sign.
The Clinical Pearl
If the mechanism is significant and the patient looks “off,” believe them. Normal vitals do not rule out critical bleeding.
Comparing External and Internal Hemorrhage
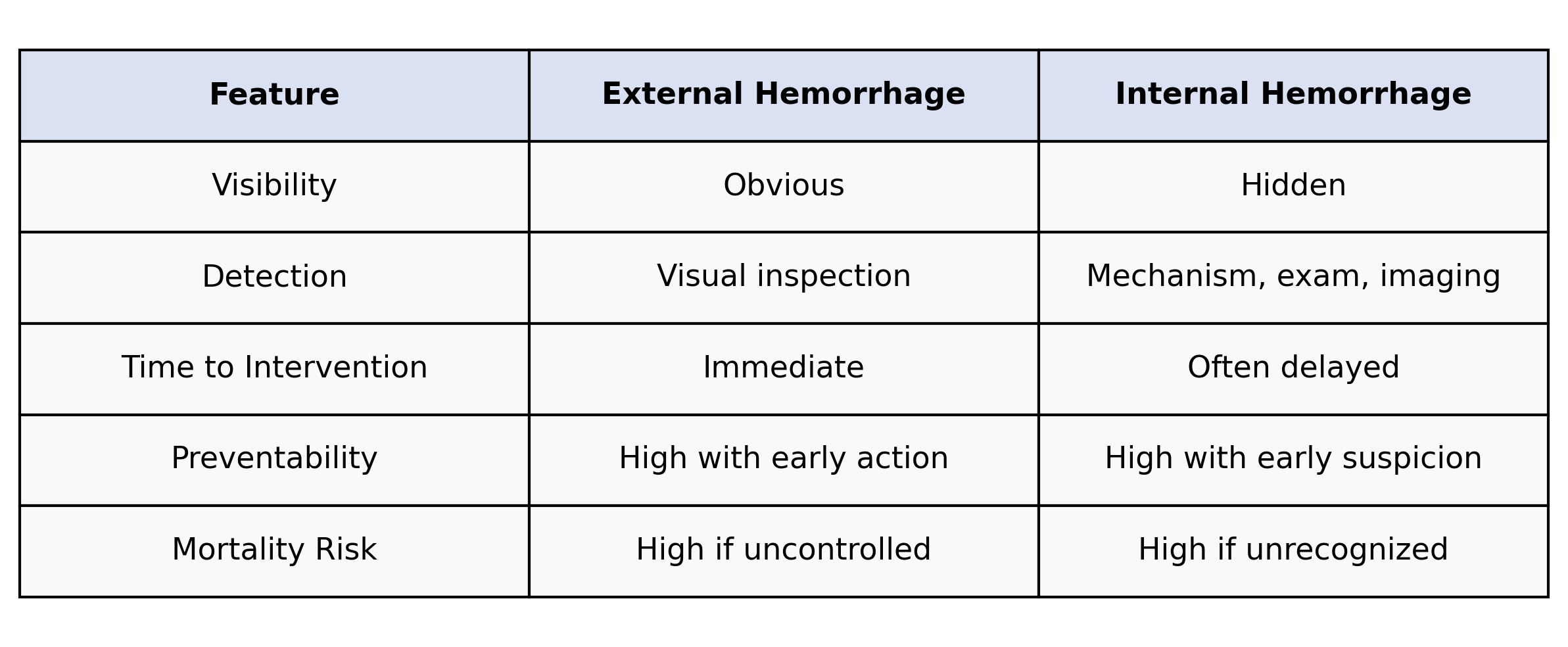
Both kill. One announces itself. The other whispers.
Awareness Is the Intervention
Modern trauma care emphasizes that hemorrhage control is not just a treatment step—it is a mindset. Damage control resuscitation and early hemorrhage identification significantly reduce mortality by targeting bleeding before physiologic collapse ensues (Schöchl, Grassetto, & Schlimp, 2013; Cannon et al., 2017).
Awareness includes:
Vigilant secondary surveys
Respect for mechanism of injury
Early use of FAST, CT, and pelvic stabilization
Rapid escalation to surgical or interventional radiology resources
In short, find the bleeding, then stop it—even when it makes you unpopular during rounds.
Call to Action: See Less. Suspect More. Act Faster.
Whether you are a nurse, physician, paramedic, or trauma educator, your awareness matters. External bleeding demands decisive action. Internal bleeding demands disciplined suspicion.
Audit your assessments. Practice hemorrhage control skills. Teach your teams to respect “normal” vital signs less and mechanisms more. Lives depend on recognizing not just the blood we see—but the blood we cannot.
Because in trauma, what you don’t see can hurt your patient far more than what you do.
References
American College of Surgeons Committee on Trauma, American College of Emergency Physicians, & National Association of EMS Physicians. (2023). Prehospital hemorrhage control and treatment by clinicians: A joint position statement. Policy Statement, 18(1), e1-e8. https://www.annemergmed.com/article/S0196-0644(23)00209-3/fulltext
Berry, C., & Fischer, P. E. (2025). Control of external hemorrhage in trauma patients. UpToDate https://www.uptodate.com/contents/control-of-external-hemorrhage-in-trauma-patients
Cannon, J. W., Khan, M. A., Raja, A. S., …Duchesne, J. (2017). Damage control resuscitation in patients with severe traumatic hemorrhage: A practice management guideline. Journal of Trauma and Acute Care Surgery, 82(3), 605–617. https://doi.org/10.1097/TA.0000000000001333
Latif, R. K., Clifford, S. P., Baker, J. A., … Bussinger, J. R. (2023). Traumatic hemorrhage and the chain of survival. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 31, 25. https://doi.org/10.1186/s13049-023-01088-8
Nickson, C. (2020). Major haemorrhage in trauma. LITFL. https://litfl.com/major-haemorrhage-in-trauma/
Schöchl, H., Grassetto, A., & Schlimp, C. J. (2013). Management of hemorrhage in trauma. Journal of Cardiothoracic and Vascular Anesthesia, 27(4 Suppl), S35–S43. https://doi.org/10.1053/j.jvca.2013.05.015
Wohlgemut, J. M., Pisirir, E., Stoner, R. S., …Tai, N. R. M. (2024). Identification of major hemorrhage in trauma patients in the prehospital setting. Trauma Surgery & Acute Care Open, 9(1), e001214. https://doi.org/10.1136/tsaco-2023-001214