
When the Beat Stops: Traversing the Worlds of Traumatic and Non-Traumatic Cardiac Arrest

Disclaimer: This article is educational and conceptual. It is not individualized medical advice.
In the high‑octane world of emergency medicine, few scenarios spike the adrenaline quite like cardiac arrest. The patient's heart has decided to take an unscheduled vacation, and our job is to convince it that the itinerary still includes a vigorous beat.
But not all cardiac arrests are created equal. We deal with two primary flavors: the “garden variety” non‑traumatic arrest—often a silent, insidious event—and the “rode hard and put away wet” traumatic arrest, which is anything but subtle. Navigating these two requires different playbooks, a shift in mindset, and an appreciation for the chaos theory of human physiology.
The Non‑Traumatic Arrest: A Rhythmic Conundrum
Imagine this: a patient in their living room suddenly collapses. The cause is likely an electrical malfunction—a wonky wire in the heart’s sophisticated circuitry.
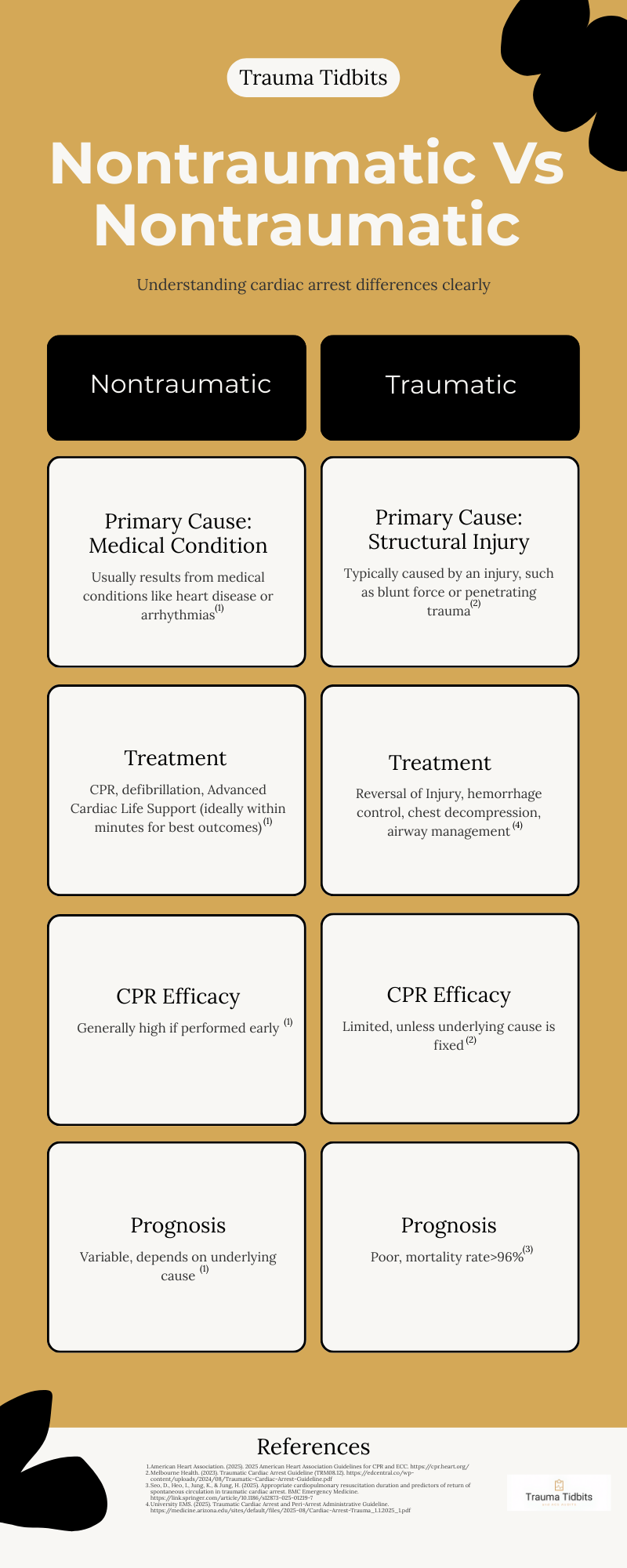
In non‑traumatic arrest, our primary protocol is a familiar dance: high‑quality CPR, early defibrillation, and advanced life support medications—an approach supported by current resuscitation science and guideline updates from the American Heart Association (AHA, 2025).
The focus is internal, targeting the heart muscle and its rhythm. The patient may have underlying coronary artery disease, a massive myocardial infarction, or significant electrolyte abnormalities. We push hard on the chest, we shock the heart, and we hope the patient’s basic physiology is intact enough to respond. This approach is standardized thanks to decades of refinement in medical arrest management.
The Traumatic Arrest: Mechanical Mayhem
Now picture this: a high‑speed motor vehicle collision, a fall from a significant height, or an unfortunate encounter with a blunt object. Here, the heart often stops not because of electrical failure but because the supporting anatomy has sustained catastrophic injury.
In such cases, CPR can feel like rearranging deck chairs on the Titanic if the underlying problem isn’t addressed first. Evidence‑based trauma guidelines note that traumatic cardiac arrest (TCA) is usually driven by reversible mechanical or volume‑related causes—massive hemorrhage, tension pneumothorax, or cardiac tamponade—rather than primary electrical dysfunction (Traumatic Cardiac Arrest Guideline, 2023).
Research consistently shows that TCA has markedly worse outcomes than non‑traumatic arrests, with mortality rates exceeding 96% (Seo et al., 2025).
Because chest compressions alone are often ineffective in TCA, guidelines emphasize restoring circulating volume, relieving thoracic obstruction, and controlling hemorrhage as top priorities, even before CPR (University EMS Guideline, 2025).
The Great Divide: Focus and Urgency
Here are the major differences:
In trauma, we have only seconds to reverse the infamous H’s and T’s. Procedures that take a back seat in medical arrest—like chest tube placement or rapid hemorrhage control—become first in line for TCA (University EMS Guideline, 2025).
The grim wit in managing a traumatic arrest is acknowledging that the world’s best CPR is useless if the patient has no blood to circulate.
The Bottom Line
Whether it’s a calm medical collapse or a chaotic trauma scene, our mission is always the same: restore life. But the path differs dramatically.
A non‑traumatic arrest is like trying to jump‑start a car with a dead battery.
A traumatic arrest is like trying to jump‑start a car that’s missing its engine.
Both demand immediate attention, but they require entirely different tools—and knowing which toolbox to open can mean the difference between a tragic ending and a fighting chance.
References
American Heart Association. (2025). 2025 American Heart Association Guidelines for CPR and ECC. https://cpr.heart.org/
Melbourne Health. (2023). Traumatic Cardiac Arrest Guideline (TRM08.12). https://edcentral.co/wp-content/uploads/2024/08/Traumatic-Cardiac-Arrest-Guideline.pdf
Seo, D., Heo, I., Jung, K., & Jung, H. (2025). Appropriate cardiopulmonary resuscitation duration and predictors of return of spontaneous circulation in traumatic cardiac arrest. BMC Emergency Medicine. https://link.springer.com/article/10.1186/s12873-025-01219-7
University EMS. (2025). Traumatic Cardiac Arrest and Peri-Arrest Administrative Guideline. https://medicine.arizona.edu/sites/default/files/2025-08/Cardiac-Arrest-Trauma_1.1.2025_1.pdf