
Mind the Gap: Practical (and Painless) PI Loop Closure Timeline Examples

Performance Improvement (PI) has matured. What once passed as “closing the loop” (a meeting note and a hopeful nod) is no longer sufficient in an era of real‑time dashboards, implementation science, and increasingly sophisticated accreditation reviews. Today, loop closure is expected to demonstrate measured change, sustained performance, and learning over time—not just good intentions.
In contemporary improvement science, loop closure is best understood as the final analytic step of iterative change, confirming that an intervention worked and that it continues to work under routine conditions (Shah et al., 2024; McNicholas et al., 2019). Timelines matter—not because speed is everything, but because improvement without temporal discipline tends to drift.
This article revisits PI loop closure timelines using practical examples that align with modern healthcare quality expectations.
What Loop Closure Means in 2026
Current trauma and hospital PI guidance defines loop closure as the documented demonstration that corrective actions resulted in improvement and reduced the likelihood of recurrence, supported by data and follow‑up review (Froedtert & Medical College of Wisconsin, 2024). Importantly, loop closure is no longer framed as a single event but as a decision point informed by post‑implementation measurement.
Recent improvement‑science literature emphasizes three essentials:
Explicit re‑measurement plans
Adequate time for signal detection
Evidence of sustainment, not just change
(Shah et al., 2024; Menon et al., 2026)
The Modern PI Loop Closure Timeline Framework
Across healthcare settings, loop closure typically unfolds in four phases:
Issue Identification & Validation – Confirm the problem is real and measurable
Intervention & Implementation – Apply a targeted, testable change
Post‑Implementation Measurement – Collect sufficient data to detect improvement
Closure Decision – Close, extend, or redesign the intervention
Recent reviews show that PI projects are more successful when timelines are tied to data sufficiency rather than calendar convenience (Menon et al., 2026; McNicholas et al., 2019).
Timeline Example 1: Documentation Compliance (Low Risk, High Volume)
Issue: Incomplete trauma team activation documentation
Risk Level: Low clinical risk
Measurement: Chart audit compliance rate
Timeline
Weeks 0–2: Issue validation and focused education
Weeks 3–6: Concurrent audits (≥20 cases)
Week 7: Compliance trending reviewed
Week 8: Loop closure determination
Why this works now:
Contemporary guidance supports short-cycle testing for high-frequency process issues when outcome risk is low and measurement is straightforward (Institute for Healthcare Improvement [IHI], 2025; Menon et al., 2026).
✅ Expected closure window: 30–60 days
Timeline Example 2: Clinical Process Reliability (Moderate Risk)
Issue: Delays in antibiotic administration for open fractures
Risk Level: Moderate
Measurement: Registry timestamps and compliance percentage
Timeline
Month 0: Root cause analysis and protocol refinement
Month 1: Education and order‑set deployment
Months 2–4: Case‑based monitoring
Month 5: Pre‑/post‑comparison
Month 6: Closure or extension decision
Why this works now:
Recent quality‑improvement studies demonstrate that 3–6 months of data is often required to distinguish true improvement from normal variation in clinical processes (Menon et al., 2026; Shah et al., 2024).
✅ Expected closure window: 3–6 months
Timeline Example 3: System‑Level or High‑Risk Events
Issue: Inconsistent activation of massive transfusion protocol (MTP)
Risk Level: High
Measurement: Multisource data (registry, blood bank, PI review)
Timeline
Months 0–1: Multidisciplinary review and pathway redesign
Months 2–3: Simulation and targeted education
Months 4–9: Case review and outcome trending
Months 10–12: Leadership review and sustainment plan
Why this works now:
High‑risk system changes require longer observation periods to confirm reliability across teams, shifts, and patient populations. Current improvement science cautions against premature closure in complex systems (Shah et al., 2024; Froedtert & Medical College of Wisconsin, 2024).
✅ Expected closure window: 6–12 months
What the Recent Literature Warns Us About
Even in 2024–2026, the most common PI failures remain remarkably consistent:
Declaring closure without re‑measurement
Using education as the sole intervention
Failing to define sustainment criteria
Large‑scale reviews continue to show that PDSA cycles are frequently documented without adequate follow‑up data, weakening conclusions about effectiveness (McNicholas et al., 2019; Menon et al., 2026).
Current Best‑Practice Timeline Benchmarks
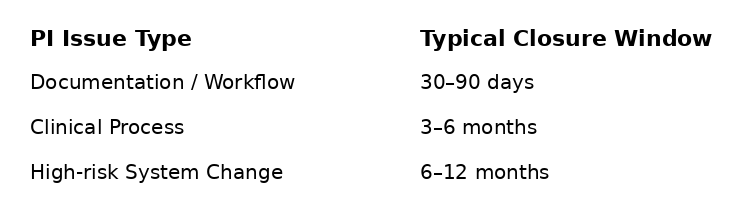
These benchmarks reflect current accreditation expectations and improvement‑science consensus, not arbitrary tradition (Froedtert & Medical College of Wisconsin, 2024; IHI, 2025).
Call to Action: Close the Loop with Confidence
Modern PI is no longer about proving you did something—it is about proving it worked, lasted, and mattered. Standardize loop‑closure timelines, define re‑measurement expectations up front, and treat closure as an evidence‑based decision, not a deadline.
Because in today’s healthcare environment, an open loop is not neutral—it’s a risk.
If your organization is ready to modernize PI timelines, strengthen closure documentation, or align improvement work with current ACS and BMJ standards, now is the time to act.
References
Froedtert & Medical College of Wisconsin. (2024). Trauma performance improvement and patient safety guidelines. https://www.froedtert.com/sites/default/files/upload/docs/services/trauma/guidelines/trauma-performance-improvement-patient-safety-guideline.pdf
Institute for Healthcare Improvement. (2025). Model for Improvement. https://www.ihi.org/library/model-for-improvement
Menon, A. A., Mudannayake, R., Bland, J., Gerrard, C., Petty, M., & Jones, N. (2026). Improving implementation of enhanced recovery after surgery using PDSA cycles. BMJ Open Quality, 15(1), e003612. https://bmjopenquality.bmj.com/content/15/1/e003612
McNicholas, C., Lennox, L., Woodcock, T., Bell, D., & Reed, J. E. (2019). Evolving quality improvement support strategies to improve PDSA cycle fidelity. BMJ Quality & Safety, 28(5), 356–365.
https://doi.org/10.1136/bmjqs-2017-007605
Shah, A., Hoffman, J. M., Twum‑Danso, N., Burlison, J., & Barker, P. (2024). Current state and future directions for improvement science. BMJ Leader, 9(3), 295–300. https://doi.org/10.1136/leader-2024-001061