
The PI Log: What to Track for Trauma Services (and Why It Matters More Than You Think)
In trauma care, excellence is rarely accidental. It is documented, reviewed, debated, re‑educated, and—eventually—improved. At the center of this continuous cycle lives a deceptively humble tool: the Performance Improvement (PI) log.
Often underestimated (and occasionally feared), the PI log is not merely a list of “who messed up.” When used correctly, it is the trauma program’s early warning system, accountability ledger, and roadmap for safer care—all in one spreadsheet (or database, if you’re living the dream).
So what should a trauma PI log actually track? And how do we ensure it supports improvement rather than becoming a compliance chore? Let’s break it down.
What Is the Trauma PI Log—Really?
The PI log is the structured record of identified variances, process failures, adverse events, and opportunities for improvement within a trauma program. According to the American College of Surgeons Committee on Trauma (ACS‑COT), it is a core component of a hospital’s continuous performance improvement process, designed to identify trends, drive corrective actions, and monitor outcomes over time (American College of Surgeons [ACS], 2022).
In plain terms:
If it’s not in the PI log, it didn’t happen—and it definitely didn’t improve.
Key Categories Every Trauma PI Log Should Track
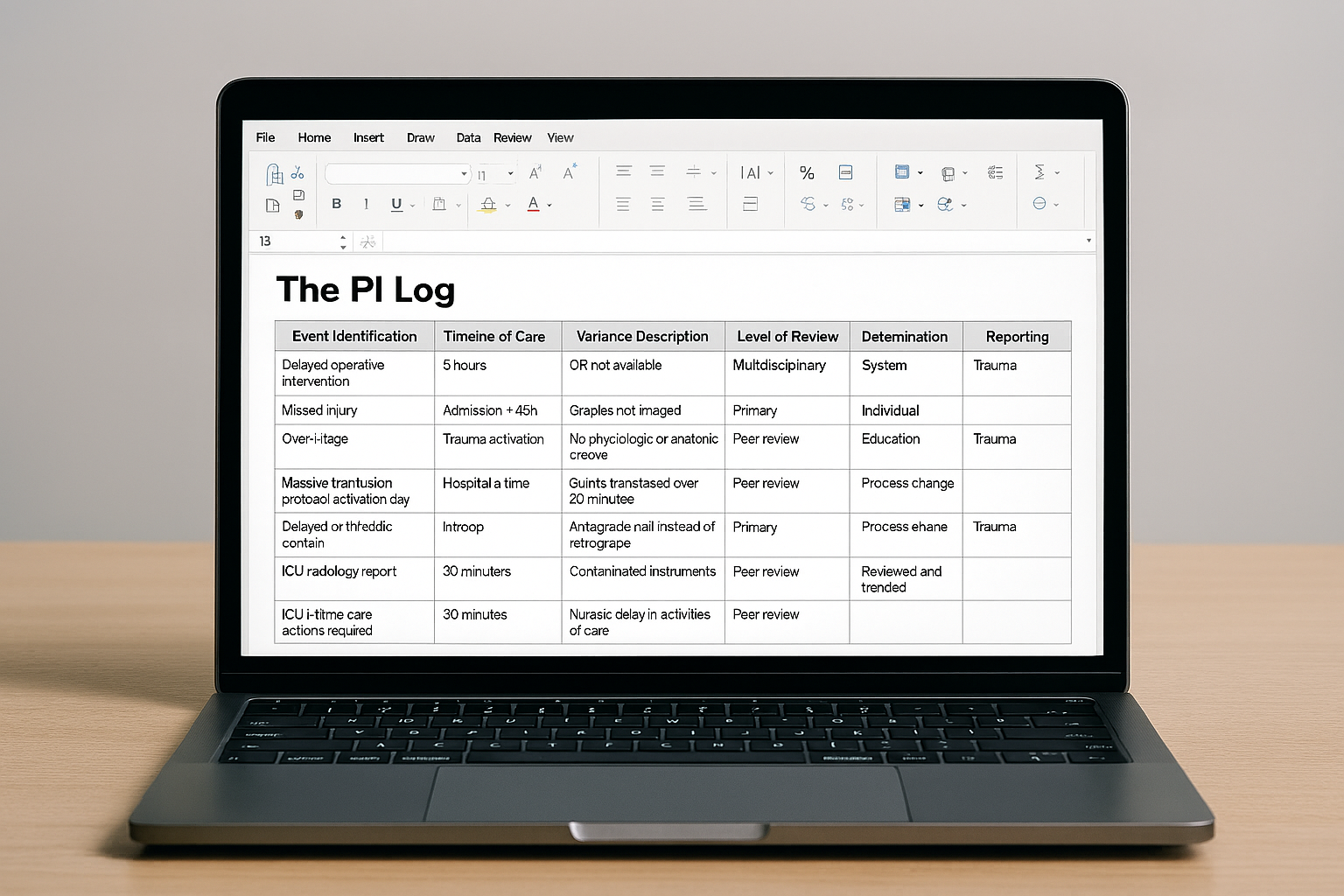
1. Event Identification
Every PI journey begins with recognizing that something deviated from expected care. This includes:
Delays in evaluation, intervention, or disposition
Protocol noncompliance (e.g., massive transfusion activation delays)
Complications or adverse outcomes
Opportunities for improvement identified via audit filters
ACS‑COT standards emphasize the use of audit filters to systematically identify cases requiring review, ensuring consistency and objectivity in PI case selection (ACS, 2022).
Pro tip: A strong PI log captures process issues, not just bad outcomes. The absence of harm does not always equal high-quality care.
2. Timeline of Care
Time is trauma’s most unforgiving variable. Effective PI logs document:
Arrival time
Time to surgeon presence
Time to imaging, blood, OR, or interventional radiology
Time to definitive disposition
Tracking these intervals allows trauma programs to identify latent system delays and benchmark performance against national data sets such as TQIP (Haider et al., 2014).
When trends emerge, they rarely whisper—they shout.
3. Variance Description
A variance is not simply “what went wrong,” but how care deviated from expected standards. High-quality PI logs include:
Clear, objective descriptions
Reference to relevant protocols or guidelines
Differentiation between human error, system failure, and unavoidable circumstances
This distinction supports a just culture framework, ensuring accountability without blame (Dekker, 2016).
4. Level of Review
Not all issues require the same level of scrutiny. PI logs should specify whether cases were reviewed at:
Primary review (trauma program staff)
Secondary review (trauma medical director)
Multidisciplinary trauma peer review committee
This tiered approach is explicitly required by ACS‑COT to ensure appropriate escalation and physician engagement (ACS, 2022).
5. Determination and Classification
After review, the outcome must be documented:
Opportunity for improvement identified (yes/no)
Classification of issue (individual, system, or both)
Preventability determination when applicable
Consistent classification enables trend analysis, which is the true power of the PI log—not the single case, but the story the cases tell together.
6. Corrective Action and Loop Closure
No PI log is complete without evidence that action followed insight. This includes:
Education or re‑education
Protocol revision
Process redesign
Equipment or staffing changes
Most importantly, trauma programs must document loop closure—confirmation that the intervention was implemented and reassessed for effectiveness (Stelfox et al., 2010).
A PI action without follow-up is just a recommendation with feelings.
7. Reporting and Trending
The PI log is not a filing cabinet. Data should be:
Aggregated and trended over time
Reported to trauma committees and hospital leadership
Used to guide strategic priorities
ACS‑TQIP benchmarking allows trauma centers to compare their outcomes and processes to national peers, strengthening both internal improvement and external accountability (ACS, 2023).
Why the PI Log Matters (Beyond Verification Visits)
Yes, a well-maintained PI log is essential for trauma verification. But more importantly, it:
Prevents recurrence of system-based errors
Supports defensible, documented improvement efforts
Enhances interprofessional communication
Protects patients—and the trauma team
In short, the PI log is where learning becomes institutional memory.
Call to Action: Make Your PI Log Work for You
Take a fresh look at your trauma PI log this quarter. Ask yourself:
Are we tracking trends—or just cases?
Are corrective actions meaningful and measurable?
Can we demonstrate true loop closure?
If the answers feel uncertain, now is the time to act. Refine your data fields, standardize your variance language, and ensure multidisciplinary ownership of the process. A strong PI log doesn’t just satisfy standards—it drives safer trauma care, one documented improvement at a time.
References
American College of Surgeons. (2022). Resources for optimal care of the injured patient. https://www.facs.org/quality-programs/trauma/quality/verification-review-and-consultation-program/
American College of Surgeons. (2023). Trauma Quality Improvement Program (TQIP). https://www.facs.org/quality-programs/trauma/quality/trauma-quality-improvement-program/
Dekker, S. (2016). Just culture: Restoring trust and accountability in your organization (3rd ed.). CRC Press.
Haider, A. H., Hashmi, Z. G., Gupta, S., Zafar, S. N., David, J. S., Efron, D. T., … Haut, E. R. (2014). Benchmarking of trauma care worldwide: The potential value of an International Trauma Data Bank (ITDB). World Journal of Surgery, 38(8), 1882–1891. https://doi.org/10.1007/s00268-014-2629-5
Stelfox, H. T., et al. (2010). Quality indicators for evaluating trauma care: A scoping review. Archives of Surgery, 145(3), 286–295. https://doi.org/10.1001/archsurg.2009.289