
The ACS Preparation Timeline: 6, 12, and 24 Months Out
A Guide for Trauma Programs on the Road to Verification
Preparing for an American College of Surgeons (ACS) verification—or reverification—can feel a bit like training for a marathon: long, rigorous, and occasionally accompanied by panicked carb‑loading. But unlike a marathon, an ACS review isn’t about the finish line; it’s about proving that high‑quality trauma care is happening every single day. A structured preparation timeline can transform the process from chaotic sprinting into a polished, predictable performance that would make even the review team smile (quietly, of course—this is still ACS).
Below is a practical, evidence‑supported roadmap to help trauma programs organize their preparation at 24 months, 12 months, and 6 months before the big site visit.
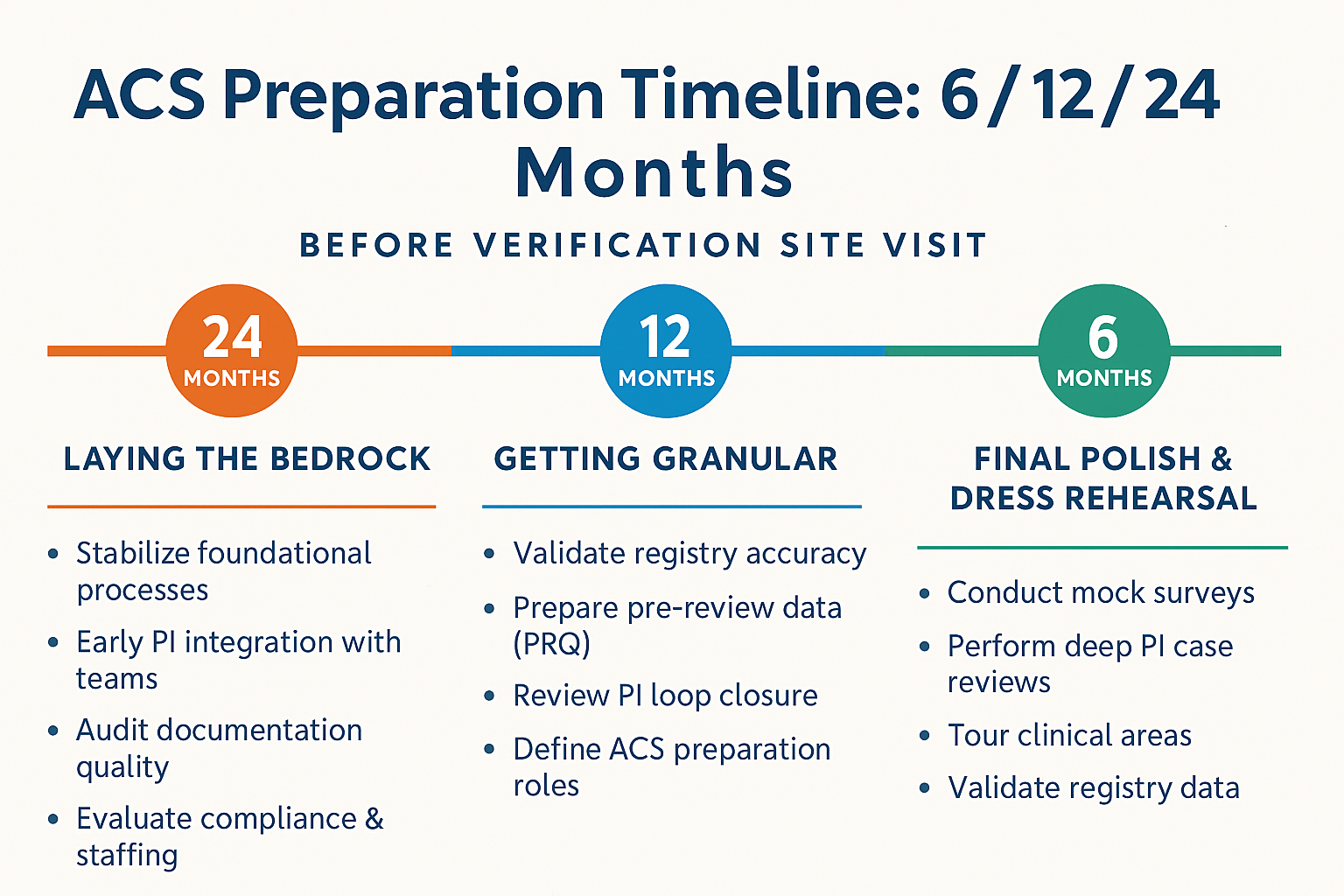
24 Months Out: Laying the Bedrock
At this stage, the focus is stabilization—of both processes and people. Trauma programs should ensure that foundational systems are aligned with ACS standards, including clinical pathways, PI workflows, credentialing, and call panel compliance. Research highlights that robust trauma system design and early integration of multidisciplinary teams lead to improved outcomes and greater readiness for verification reviews (American College of Surgeons, 2022).
This is also the ideal time to audit documentation quality, evaluate compliance with critical measures, and identify gaps in staffing or training. Although 24 months feels far away, programs that start early typically experience fewer last‑minute crises (and fewer emergency pizza-fueled chart reviews).
12 Months Out: Getting Granular
At the one‑year mark, the focus shifts to refinement. Your team should be reviewing Performance Improvement (PI) loop closure rates, trauma registry validation, peer review minutes, and clinical care metrics with a microscope that would make a pathologist proud. Evidence shows that consistent quality review cycles and well-documented PI processes significantly strengthen verification performance and long-term patient care outcomes (Young, 2021).
Now is also the time to build or update your Pre‑Review Questionnaire (PRQ) data. While glamorous it is not, the PRQ is essentially your trauma program’s autobiography—warts, wins, and workflows included. Keeping it accurate and clean at this point will save countless hours later.
Your ACS prep committee should be meeting routinely, roles should be clearly defined, and—most importantly—no one should be hearing the phrase “site visit” for the first time.
6 Months Out: Final Polish and Dress Rehearsal
At this point, you’re not building the house—you’re decorating it. Conduct mock surveys, perform deep PI case dives, and finalize documentation that demonstrates compliance with ACS standards. Mock reviews improve team readiness and reducing onsite deficiencies in any survey (Radeker, n.d.).
Walking tours of clinical areas, quick‑response drills with staff, and final validation of registry data are essential. This is also the time to ensure that everyone—from the trauma medical director to the person answering the ED phone at 0200—knows what the ACS is, why they’re coming, and how they contribute.
With 6 months to go, the goal is confidence, clarity, and smooth coordination—like a trauma resuscitation, but with fewer chest tubes.
Conclusion: A Prepared Trauma Program Is a Powerful One
ACS verification isn’t a one‑day assessment—it’s a reflection of everyday practice. By approaching the process through a structured 24‑/12‑/6‑month timeline, trauma programs can ensure that they’re not just ready for verification—they’re ready for excellence. And while no survey is completely without surprises, disciplined preparation helps ensure that any surprises are minimal, manageable, and (ideally) unrelated to missing documentation.
If your trauma program is preparing for ACS verification, don’t wait.
Start now. Build your timeline. Engage your team.
And if you want help creating tools, checklists, education packets, or mock survey materials—I’m here to help you elevate your preparation from “good” to “ACS‑ready.”
References
American College of Surgeons. (2022). Resources for optimal care of the injured patient (7th ed.). https://www.facs.org/quality-programs/trauma/quality/resources/
Radeker, T. (n.d.). Gearing up for success— A new trauma program manager’s guide to mastering their first trauma survey. Optimal Healthcare Advisors. https://oha-llc.com/a-tpms-guide-to-mastering-their-first-trauma-site-survey/
Young, J. S. (2021) Trauma center performance improvement. Springer. https://doi.org/10.1007/978-3-030-71048-4