
Circulation – Early Signs of Shock in Trauma Patients
Understanding Shock in Trauma
Trauma is the leading cause of shock in emergency settings, primarily hypovolemic shock due to hemorrhage. However, trauma can also cause obstructive shock (e.g., tension pneumothorax), cardiogenic shock (e.g., cardiac contusion), or distributive shock (e.g., spinal cord injury).
Key Concept:
Shock in trauma is often occult—patients may appear stable while compensatory mechanisms mask severity (Vincent & De Backer, 2013; Guyton & Hall, 2021). Waiting for hypotension is too late.
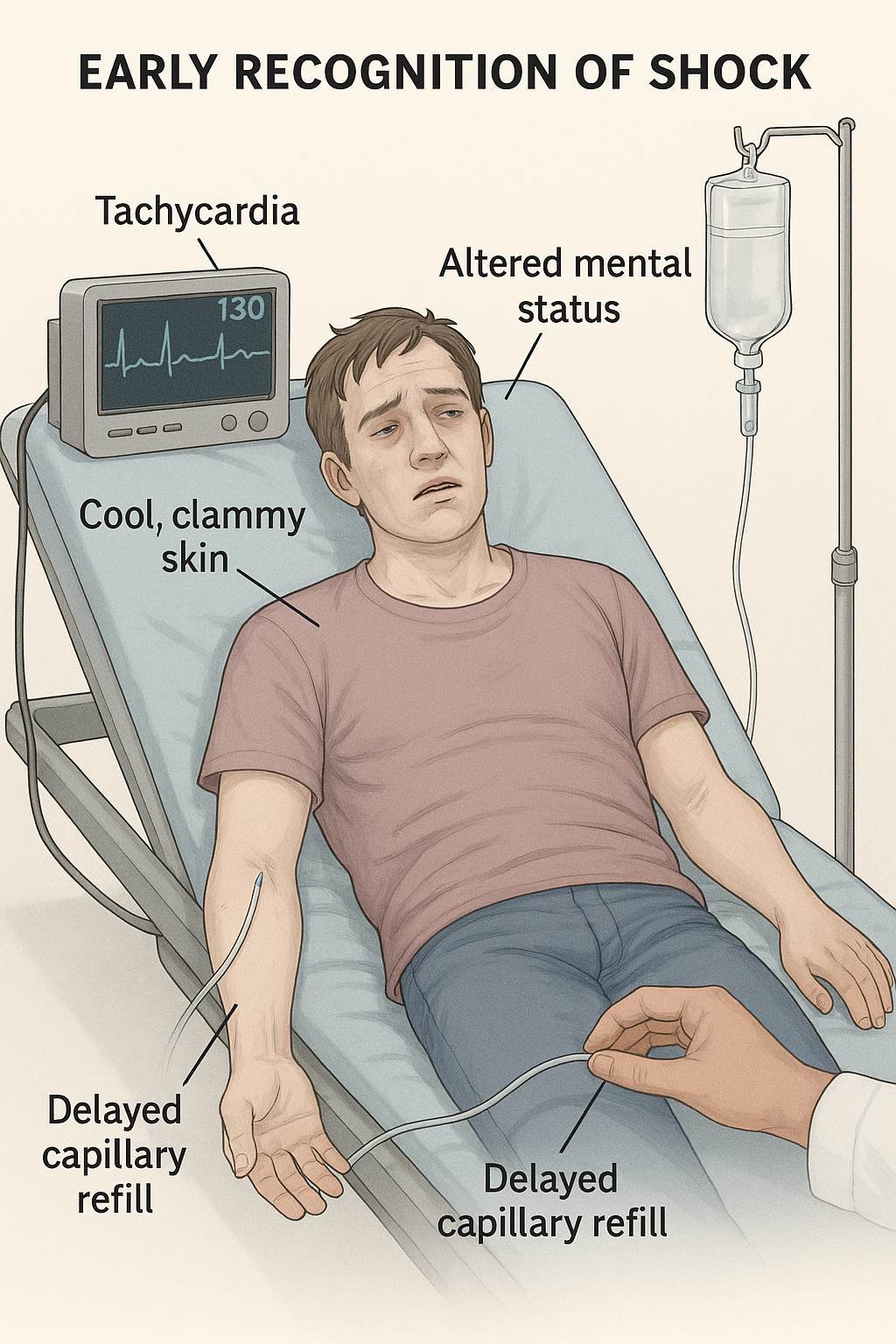
Early Signs of Shock in Trauma
Compensatory Phase Indicators
Tachycardia: First and most reliable sign in trauma (American College of Surgeons, 2022).
Cool, clammy skin: Peripheral vasoconstriction to maintain core perfusion.
Narrowing pulse pressure: Systolic may remain normal while diastolic rises.
Subtle mental status changes: Anxiety, agitation, or restlessness—often dismissed as emotional response to trauma.
Delayed capillary refill: >2 seconds is concerning.
Clinical Pearl:
Do not rely solely on blood pressure. A trauma patient with normal BP can still be in Class II shock (15–30% blood loss) (American Heart Association, 2023).
Trauma Case Scenarios
Case 1: The Motorcycle Crash
Patient: 28-year-old, motorcycle collision, HR 122 bpm, BP 130/84, skin cool and pale, cap refill 3 sec, anxious.
Question: What is happening?
Discussion: Despite normal BP, tachycardia and poor perfusion indicate early hypovolemic shock.
Action: Activate massive transfusion protocol, apply direct pressure to bleeding sites, monitor urine output.
Case 2: The Hidden Hemorrhage
Patient: 40-year-old, blunt abdominal trauma, HR 110 bpm, BP 128/80, skin clammy, slightly confused.
Question: Is this shock?
Discussion: Yes—likely internal bleeding. Mental status change and tachycardia are key.
Action: Rapid imaging (FAST), IV fluids, prepare for OR.
Case 3: The Chest Trauma
Patient: 55-year-old, chest wall injury, HR 108 bpm, BP 135/90, cool extremities, diaphoresis, muffled heart sounds.
Question: What’s the risk?
Discussion: Early obstructive or cardiogenic shock (possible tamponade).
Action: Oxygen, cardiac monitoring, prepare for pericardiocentesis.
Quick Recognition Checklist for Trauma
HR > 100 bpm?
Skin cool/clammy or delayed cap refill?
Pulse pressure narrowing?
Mental status changes?
Mechanism suggests hidden bleeding?
If YES to any, act now—don’t wait for hypotension.
Conclusion
Every second counts in trauma care.
Train your eyes to see beyond the numbers. Recognize the whispers of shock before they become screams. Document findings, escalate care, and advocate for rapid intervention. Your vigilance saves lives.
References
American College of Surgeons. (2022). Advanced trauma life support (ATLS®): Student course manual (10th ed.). Chicago, IL: American College of Surgeons. https://doi.org/10.1097/TA.0000000000003659
American Heart Association. (2023). Circulatory shock: Recognition and management guidelines. https://www.heart.org/en/professional
Guyton, A. C., & Hall, J. E. (2021). Textbook of medical physiology (14th ed.). Elsevier. https://doi.org/10.1016/C2018-0-00298-1
Vincent, J. L., & De Backer, D. (2013). Circulatory shock. New England Journal of Medicine, 369(18), 1726–1734. https://doi.org/10.1056/NEJMra1208943